Having an ERCP
(Endoscopic Retrograde Cholangio Pancreatography)
What is an Endoscopic Retrograde Cholangio Pancreatography (ERCP)?
An ERCP is a type of X-ray and camera examination that enables your doctor to examine and/or treat conditions of the biliary system (liver, gall bladder, pancreas, pancreatic and bile ducts).
To perform the test, a flexible tube about the width of an index finger with a tiny camera on the end of it (a duodenoscope) is passed over your tongue, down your food pipe (oesophagus), through your stomach, and into the small bow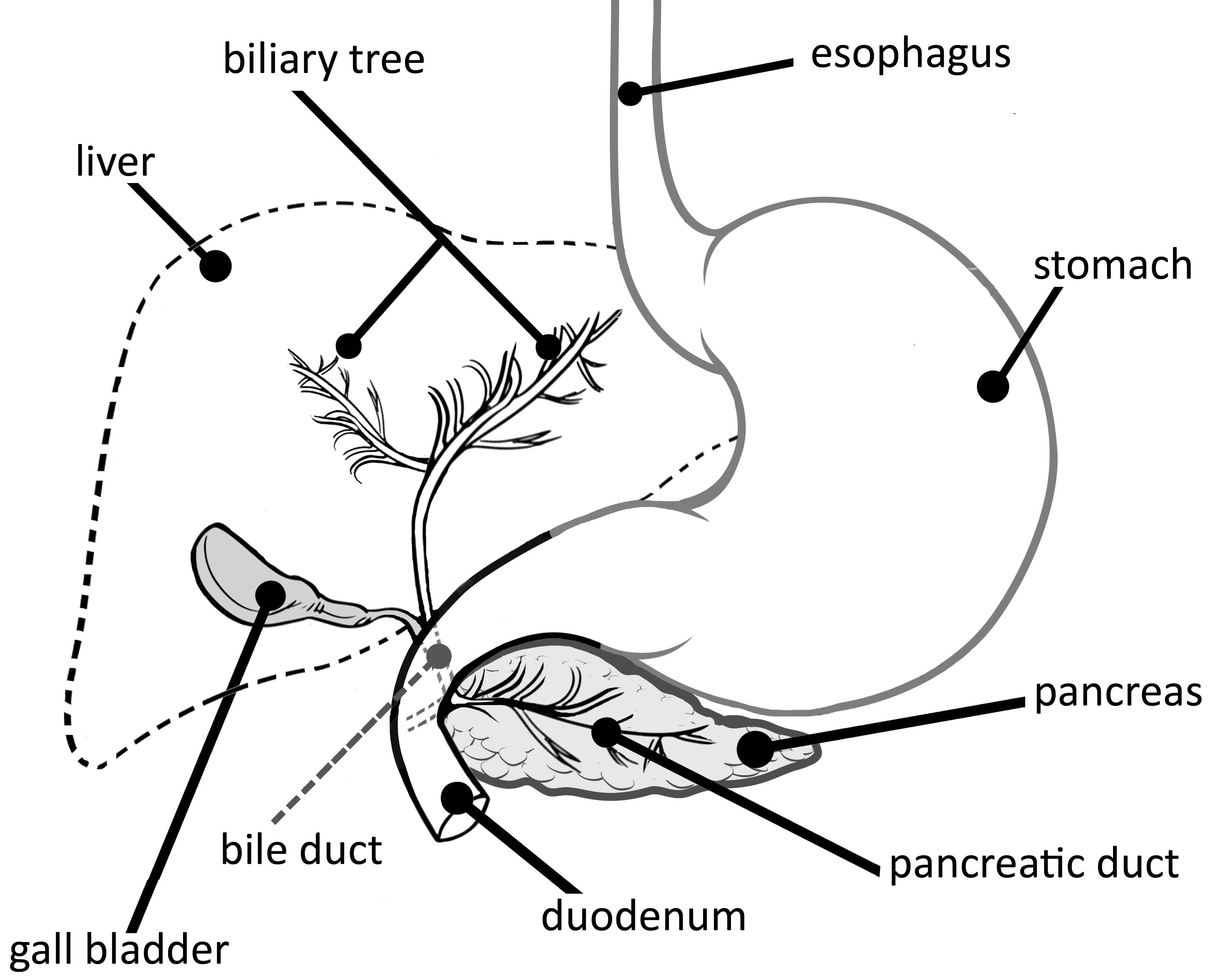 el (duodenum).
el (duodenum).
The most common reasons to have an ERCP are jaundice (yellowing of the skin or eyes) or abnormal liver function tests, especially if you have pain in the abdomen, or if a CT scan or ultrasound shows a blockage of the common bile duct or pancreatic duct. Blockages can be caused by stones, narrowing of the bile ducts (strictures), and growths of the pancreas and bile ducts.
What should you expect?
The preparation:
One week before you have the ERCP, you must attend your GP practice for blood tests to check the clotting of your blood (INR), your full blood count (FBC) and liver function (LFT). Please read your appointment letter carefully as it contains important information regarding medications and medical conditions.
You must not eat anything for at least six hours before your ERCP. You can drink clear fluids like water (no milk) up to two hours before your test. Please wear loose comfortable clothing and avoid wearing underwired bras, clothing with zippers or metal buttons as this procedure is performed under X-ray.
Admission:
When you arrive please book in at the Endoscopy reception area. Your appointment time given is the beginning of your time in the department. Please be prepared to be in the department four to six hours.
A nurse will explain the examination to you. If you have any concerns or questions at this stage don’t be afraid to ask.
The nurse will ask about your medical history and admit you for your ERCP.
Your formal consent is required before the examination can be carried out. The doctor will speak to you before the procedure to discuss the risks and benefits of having the ERCP. Consent will be obtained for an anti-inflammatory suppository to be given to you either before or after the procedure to reduce the risk of developing pancreatitis. If you understand and agree to undergo the procedure, you will be asked to sign a consent form.
During the test:
Before the procedure starts, you will be given a local anaesthetic throat spray to help to numb the throat. A nurse will attach observation monitoring equipment to record your pulse, oxygen levels and blood pressure throughout the procedure. You will need to lie on your left side with your left arm behind your back as you will be turned to lie on your front during the test. A small plastic mouth guard will be placed between your teeth to protect them. (If you have dentures you will be asked to remove them first.) Oxygen will be given via a small sponge into your nose throughout the procedure.
Medications will be injected, through a small tube (cannula) in your arm or hand, to relax you and relieve any discomfort that you might experience. These medicines (known as conscious sedation), will relax you and may make you drowsy but will not necessarily put you to sleep. You will hear what is said to you and be able to respond to any instructions.
Once you are drowsy, the camera (duodenoscope) will be passed through your mouth, down your gullet, into the stomach, and then into the top part of the small intestine (duodenum). During the procedure, the doctor will insert a fine wire into the bile ducts and inject dye, which shows up on X-ray. X-rays of various parts of your biliary or pancreatic system will be taken. Any saliva will be cleared from your mouth using a plastic suction tube.
If the procedure is being performed to remove stones from the bile or pancreatic duct, a small cut (sphincterotomy) may be made in the lower end of the bile duct to allow a fine tube to pass through. This also allows a small basket or balloon to be inserted to grasp a stone, and for any stones that may get into the bile duct in future to easily pass into the intestine.
During the test (continued):
Specimens (a small sample of tissue) may be taken from the bile ducts using a small brush or forceps, and a plastic or metal tube (stent) may be inserted to help with the drainage of bile or pancreatic juice.
After the examination:
Once the examination is finished you will be transferred to the recovery ward. The nurse will monitor your blood pressure, heart rate, temperature and oxygen levels regularly. You will need to stay in the Endoscopy Unit for four to six hours until you are fully awake and show no signs of having any complications. You will be given a drink before discharge, be able to start a light diet later the same day, and continue a normal diet the following day.
You will be given the results of your procedure before you go home and will also be told if you need any further appointments. You will also be given a written copy of the results as the sedation can make you forgetful.
As you have had sedation you will need a friend or family member to collect you and stay with you for 24 hours after the procedure. You may feel fully alert however, the sedation remains in your system for 24 hours and you may feel sleepy and forgetful during that time.You must not drive, operate machinery or drink alcohol in that time. The nurses on the ward will tell you when you are able to eat and drink.
Are there any alternatives?
It is important to understand that ERCP is usually not a simple diagnostic procedure but is performed as a alternative to open surgery. There is a complication rate of 5 to 7% (see risks of the procedure on the next page).
Risks of the procedure:
It is important to understand that ERCP carries a 5 to 7% complication rate
There is a small risk of damage to dental work and you may experience a sore throat for a day or two after the procedure.
Aspiration: Caused by inhaling liquid or choking on vomit, leading to inflammation of the lungs.
Sedation: Occasionally patients may have a reaction to the medication used. They can cause problems with breathing, heart rate and blood pressure. You will be monitored closely during the procedure to ensure any problems are recognised and treated promptly. Patients with significant health problems such as breathing difficulties or heart problems, may be assessed by a doctor or specialist nurse before the procedure.
If a sphincterotomy is performed (a cut to enlarge the opening of the bile duct) there is a risk bleeding may occur, this can be dealt with at the time by the endoscopist. Rarely bleeding can develop later. A warning sign of this is the passage of black bowel motions in the first 24 - 48 hours after the procedure.
Inflammation of the pancreas: Pancreatitis (3.5%) and perforation (0.5%) present with increasing abdominal pain usually within the first few hours after ERCP.
Sepsis or infection: (1%) causes fever, sweating, and sometimes uncontrollable shaking or rigors and can require antibiotic therapy.
Some of these complications may require admission to hospital, further scans or treatments. Rarely, an operation and longer admission to the Intensive Care Unit (ICU) may be necessary to manage a life-threatening complication. Very rarely, such complications can result in death. Risks vary depending on why the test is being performed, what is found during the procedure, what treatment is undertaken, and if you have any other health problems.
Sometimes the doctor may be unable to complete the procedure due to previous surgery on the stomach, or the effects of certain diseases on the upper bowel. You will have the opportunity to discuss the benefits, risks, and alternatives to ERCP with a doctor prior to your procedure.
If you develop increasing abdominal pain, vomiting, fever, or black bowel motions within the first 48 hours following ERCP, it is essential that you telephone 111 to seek urgent medical advice (24 hour health advice service), telephone the Endoscopy Department for advice, or alternatively return to the hospital Emergency Department promptly for investigation and treatment.
Checklist:
- Please let us know if you cannot attend your appointment so we can give it to someone else.
- Follow your instructions regarding eating and drinking before your appointment.
- Bring an up to date list of medications.
- Please contact us one week prior to your appointment if you take Warfarin, Clopidogrel, Rivaroxiban, Dabigatran, Apixaban or any other tablets to thin your blood.
- If you are diabetic please contact your practice / diabetic nurse for advice regarding your medication.
- Write down any questions / concerns.
- If you need information in your own language or an interpreter including sign language please contact the Endoscopy Unit.
- Please ensure one finger is free of nail polish or false nails.
Contact Details
Royal Lancaster Infirmary: telephone 01524 591433
Furness General Hospital: telephone 01229 403618 or 01229 402960
Please phone between 9am and 6pm if you have any queries or concerns and a member of staff will be happy to answer any questions.
Date of publication: 09/01/2026
Reference code: PIL080/PIL057
Review date: 01/01/2029